
Texten utforskar anledningen till den känsla av välbefinnande som många upplever efter manuella behandlingar som massage. Det är en vetenskapligt baserad artikel som ifrågasätter den tidigare allmänt accepterade uppfattningen om endorfiners roll i detta välbefinnande, särskilt gällande "runner's high". Istället presenterar artikeln forskning som pekar på endocannabinoider, som anandamid, som en potentiell förklaring till de positiva effekterna av både ansträngande träning och olika former av kroppsbehandling, inklusive dess smärtlindrande och antiinflammatoriska fördelar. Tillsammans belyser källorna både den praktiska tillämpningen av kroppsbehandlingar och den underliggande vetenskapliga förklaringen till deras fördelar.
1. Darmani N, et al. Involvement of the cannabimimetic compound, N-palmitoyl-ethanolamine, in inflammatory and neuropathic conditions. Neuropharmacology. June 2005;48(8):1154-63.
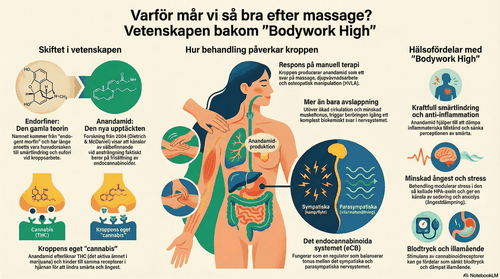
2. Dietrich A, McDaniel W. Endocannabinoids and exercise. Br J Sports Med. Oct. 2004;38(5):536-41.
3. Goldstein A, Lowery P. Effect of the opiate antagonist naloxone on body temperature in rats. Life Sci. Sept. 1975;17(6):927-31.
4. Field T, et al. CFS: massage therapy effects depression and somatic symptoms in CFS. Journal of Chronic Fatigue Syndrome. 1997;3(3):43-51.
5. Hinton E, Taylor S. Does placebo response mediate runner’s high? Percept Mot Skills. June 1986;62(3):789-90.
6. Hou C-R, et al. Immediate effects of various physical therapeutic modalities on cervical myofascial pain and trigger-point sensitivity. Arch Phys Med Rehabil. Oct. 2002;83(10):1406-14.
7. Ikimi F, et al. Interstitial fluid plasma protein, colloid, and leukocyte uptake into initial lymphatics. J Appl Physiol. Nov. 1996;81(5):2060-7.
8. Lederman E. Science and Practice of Manual Therapy, 2nd Ed. New York, Edinburgh: Churchill Livingstone, 2005.
9. McPartland J, Pruitt P. Side effects of pharmaceuticals not elicited by comparable herbal medicines: the case of tetrahydrocannabinol and marijuana. Altern Ther Health Med. July 1999;5(4):57-62.
10. McPartland J, et al. Cannabimimetic effects of osteopathic manipulative treatment. J Am Osteopath Assoc. June 2005;105(6):283-91.
11. McPartland J, Simons D. Myofascial trigger points: translating molecular theory into manual therapy. J Manual Manipulative Therapy, 2006;14(4):150-7.
12. Oschman JL. Energy Medicine: The Scientific Basis. New York, Edinburgh: Churchill Livingstone/Harcourt Brace, 2000.
13. Pertwee R. The therapeutic potential of drugs that target cannabinoid receptors or modulate the tissue levels or actions of endocannabinoids. AAPS J. Oct. 24, 2005;7(3):E625-54.
14. Simantov R, Snyder S. Morphine-like peptides in mammalian brain: isolation, structure elucidation, and interactions with the opiate receptor. Proc Natl Acad Sci USA. July 1976;73(7):2515-9.
15. Vernon H, et al. Spinal manipulation and beta-endorphin. J Manipulative Physiol Ther. June 1986;9(2):115-23.
Det är fascinerande att se hur den biokemiska forskningen nu förklarar det som mina kunder i London och Göteborg har upplevt i åratal – den där nästan euforiska känslan av lugn och harmoni efter en djupgående massagebehandling. Att förstå att vi faktiskt påverkar kroppens eget 'lyckosystem' gör mitt arbete som massageterapeut ännu mer meningsfullt.
Daniel Näsman
Medicinsk Massageterapeut @ Massageterapeuten Göteborg